 Dear Colleague:
Dear Colleague:
With the reduction in TB cases leveling off, increasingly difficult TB cases to manage, and shrinking budgets, advocacy for sufficient resources will be important to prevent another TB resurgence. We recently had an opportunity to highlight the TB problem and GTBI’s response in the Summer issue of the New Jersey Medical School’s magazine, Pulse (page 28-29).
We are pleased to report in this issue another successful “on the road” training course—this time on TB Case Management in two locations in Maine. In addition to being accessible to staff across the state, the course’s success was due largely to the strong collaboration with Maine’s TB and public health nursing programs and the use of local staff as faculty.
We also report on GTBI’s hosting of the national TB Expert Network Conference, a web-based seminar held on May 13th. This was the first in a series of conferences to be held bimonthly by the RTMCCs, CDC, and the National Jewish Medical Research Center on a rotation basis. They provide a forum for TB experts to discuss complicated cases and foster education and capacity building among TB program consultants. TB medical consultants in TB programs in the Northeastern RTMCC consultants in TB programs in the Northeastern RTMCC are always invited to attend and will be able to view archived conferences.
This issue also includes articles on The Historical Contribution of Behavioral/Social Science to TB Control and on GTBI’s updated monograph: Guidelines for the Diagnosis of Latent TB Infection in the 21st Century. Finally, this issue features an informative profile of Dr. John Bernardo, TB Medical Officer for Massachusetts and a nationally recognized leader and researcher in TB control efforts.
And, as usual, if you have any feedback for any of us, on any TB related topic, I invite you to contact me or a member of our RTMCC staff at (973-972-3270)
Lee B. Reichman, MD, MPH
Executive Director
Northeastern RTMCC and the
Global Tuberculosis Institute
back to top
TB Case Management - The Maine Perspective
In June 2008, the NJMS GTBI and the Maine Center for Disease Control and Prevention held two one-day trainings for public health nurses in Maine. These trainings were the result of collaboration that was kicked off in early 2008, when GTBI and the Maine CDC TB staff began to meet regularly via conference calls to plan a TB training in Maine. The GTBI offers a well established two-day interactive skills building workshop on nurse case management in Newark; however, as the initial planning for the Maine training began, it was quickly determined that this course would need to be adapted when “taken on the road’ to Maine. To begin with, the nurses in Maine would only be able to attend a one-day course and their preference was a format that included panel discussions and case presentations, rather than the role playing and other activities included in the course offered in Newark. Additionally, since Maine is such a geographically large state, to make this course accessible to as many public health nurses as possible, the team decided to offer the course in two separate locations, Bangor and Augusta.
The planning committee for the course included members of the TB control program, public health nursing supervisors, and RTMCC staff; this mixed composition allowed for multiple perspectives and insight into the challenges encountered in TB control and prevention in Maine. Specific interests identified were TB in the pediatric population and cultural competency. The Maine contingent also really wanted to explore the role of the Nurse Case Manager in specific instances, and focus on working together to address the common challenges in TB case management.
The courses were held June 18th and 19th 2008; there were twenty-three attendees in Bangor and twenty-seven in Augusta. As with all GTBI offsite trainings, the TB Program and other state Health Department staff played an integral role. The training began with a session we called “Interaction of Public Health Nurses & Maine TB Program.” Joyce Roy, Public Health Nurse Consultant; Anne Sites, Sr. Health Program Manager; and two PHN Supervisors, Jane McQuarrie and Steve Garacia, coordinated that session. They discussed challenges that occur when public health field nurses are case managing a patient with tuberculosis and provided clarification on how the programs are integrated.
Three unique sessions were organized for this course. They were “Cultural Issues Facing TB Case Managers,” “Challenges in TB Case Management,” and “Pediatric Tuberculosis.” Each session began with an exercise or case study and was followed by a panel discussion. The panels were comprised of nurses from Maine and RTMCC staff including DJ McCabe, Nurse Educator; Lillian Pirog, Nurse Manager; and Nisha Ahamed, Program Director for Training and Education.
During the first session, some of the cultural issues identified were religious beliefs and traditions, beliefs about the efficacy of BCG vaccine, and the use of interpreters. The session began with an exercise that focused on qualities and traits that may or may not be immediately apparent and how these influence how a person views the world and makes decisions. In addition to questions from the participants, panelists used vignettes to address areas of interest and generate additional discussion. This format was also used for the sessions that followed.
In the Challenges to TB Case Management session, topics included treatment adherence, discharge planning, legal issues, maintaining competency in low-incidence areas, and documentation. Pam Correll, Informatics Consultant, addressed ways that data collected in the field are used by the TB Program and the advantages of CareFacts, the information system platform used by the Maine CDC.
The Pediatric Tuberculosis session began with an introduction by Dr. Kathleen Gensheimer, the TB Program Medical Director, who presented the epidemiology of TB in children in the state of Maine. This was followed by an overview of the management of pediatric TB by Lillian Pirog, Nurse Manager and Pediatric Nurse Practitioner at the Global TB Institute.
The highlight however, were the two cases presented by Maine public health field nurses. Pam Harpine, PHN presented the case of her patient who was a migrant worker who presented with TB while he was employed as a potato packer in Maine. Jean Hall, PHN shared the case of a foreign-born infant with tuberculosis who had been adopted by a family in Maine. The audience especially enjoyed hearing from their colleagues and each of these cases helped keep the focus on locally pertinent issues.
Thanks to the strong collaboration with the Maine TB and public health nursing programs, the courses were very successful! All participants agreed or strongly agreed that the course identified practical case management strategies to address challenges, and more than 92% of participants agreed or strongly agreed that course objectives were met. Taking a course “on the road” often causes the GTBI Education & Training staff to “think out of the box” and experiment with new techniques. The Maine experience was no exception to this!
Submitted by DJ McCabe, RN Nurse Educator NJMS Global Tuberculosis Institute
back to top
The Historical Contribution of Behavioral/ Social Science to TB Control
Tuberculosis has long and famously been described as a “social disease with a medical aspect that progresses only when its ‘seed’ (bacillus M tuberculosis) is established in the fertile ‘soil’ of poverty, hunger, and deprivation.” These words from William Osler are as true today as they were when he spoke them one hundred years ago (Rosenkrantz 1994).
The behavioral and social sciences can be and have been of assistance to TB control in many ways. In general, behavioral/social science inquiry can increase our understanding of patients’ thoughts and behaviors – what motivates them to get tested, start treatment, and remain adherent. Building on this knowledge, the behavioral and social sciences can assist in designing interventions to change behavior. Behavioral/social science research often focuses on cultural factors, assessing patient knowledge and attitudes, and addressing the specific needs of such high-risk groups as the homeless, substance abusers, and immigrants. Over time, many of the individuals conducting research have not had behavioral or social science backgrounds – they have simply been trying to uncover information necessary for better TB control.
Discussions of TB control in the U.S. often begin with the late 1800s and Hermann Biggs, a prominent figure in the development of modern public health policy and institutions in New York (Journal of Public Health Policy 1985). As Frieden and colleagues (2000) point out, there is a surprising consistency over the past century in the most pressing concerns in TB control. With the exception of the impact of HIV, the issues are the same: the heightened vulnerability of, and the challenges inherent in treating the poor, substance abusers, and immigrants.
Similarly, Biggs’ strategies for TB control endure and are reflected in the World Health Organization’s promotion of DOTS — microscopy, efforts to stop transmission, best available treatment combined with case management, reporting and follow-up, and political will. Of course, some of these strategies now take very different forms. In the late 1800s and early 1900s, the best available “treatment” was nutritional support, cough etiquette, rest, and isolation, while now it is uninterrupted chemotherapy. Case management formerly consisted principally of education through nurses visiting patient’s homes; now case management also encompasses ensuring adherence to treatment (e.g., through Directly Observed Therapy) and contact investigation.
One researcher who brought a psychosocial focus to TB work was Thomas Holmes (Lerner 1996). Dr. Holmes was a physician, trained in infectious diseases. After doing a fellowship in psychosomatic medicine, he took a staff psychiatrist position at Firland, a TB sanatorium in Seattle, Washington.
Holmes (whose TB research was conducted between 1949 and 1961) had an interest in the impact of stress on TB. An early study examined the relationship between progress of TB disease and stress, as measured by urinary 17-ketosteroid levels. A subsequent study examined stressful events in Firland employees. Those who developed TB were more likely to have unstable lifestyles, emotional and economic problems, and a lack of close interpersonal relationships. A third study looked at psychological and social factors in recovery from TB and found that treatment failure was associated with male sex, old age, co-existence of non-TB illnesses, and hospital discharge against medical advice (Lerner 1998).
The work of Holmes and his colleagues certainly suffered from methodological flaws and concerns about causative direction (e.g., is stress causing disease or is it the result of disease?). From the perspective of a halfcentury later, the measurement of psychological factors was in its infancy. As Lerner (1996) points out, this fledgling interest in psychological issues dissipated with the use of new antibiotics that cured more patients with a shorter course of therapy. However, the spirit of Holmes’ work lives on today in the field of psychoneuroimmunology, and the growing attention on the “mind-body” connection.
TB control in the 1950s was also the locus for the development of one of the first theoretical models to explain patient behavior, the Health Belief Model (HBM). This theory is still widely taught in schools of public health and is used in design of public health interventions.
Godfrey Hochbaum, a psychologist, conducted a study of knowledge, attitudes, and behavior in relation to people agreeing to be X-rayed in mobile X-ray vans (Hochbaum 1956). He found that people were more likely to accept the X-ray if: 1) they believed they might get TB, 2) they knew that the presence of symptoms was insufficient to diagnose TB, and 3) they believed that it was better to detect the disease early. These findings later evolved into foundational elements of the HBM, including the concepts of susceptibility, severity of disease, perceived effectiveness, costs and benefits, and ‘cues to action’ that spur patients to take action that they believe will benefit them personally.
In this early examination of knowledge and attitudes, Dr. Hochbaum distinguished between knowledge and beliefs, and also between knowledge and behavior. Interestingly, he noted the limitations of relying too much on merely providing information to patients: “What we are dealing with here is not merely a matter of information. It is a matter of real belief and of a conviction on the part of people that such information applies to them personally and that it is important to them as individuals. Without question, a person must know what to do, when to do it, and how to do it before he can take action. But merely knowing these things will usually be insufficient to elicit the action to which they relate.” From a public health standpoint, this information can help TB staff develop educational messages that are more likely to affect patient behavior.
This intersection of biology and human society continues to inspire behavioral and social inquiry in social scientists and health practitioners alike. In the next issue, we will explore the contribution of the behavioral/social sciences in the fight against HIV/AIDS and its implication for TB control.
CITATIONS Frieden TR, Lerner BH, Rutherford BR, “Lessons from the 1800s: tuberculosis control in the new millennium” The Lancet 355:1088-1092. (Mar 25, 2000) Hochbaum GM. “Why people seek diagnostic XRays” Public Health Reports 71 (4):377-380. April 1956. Journal of public health policy “Models for public health workers: Charles V. Chapin, Hermann M. Biggs, and Joseph W. Mountin” (Sep 1985). 6 (3): 300–6 Lerner BH, “Can stress cause disease? Revisiting the Tuberculosis research of Thomas Holmes, 1949-1961” Annals of Internal Medicine 124(7):673-680. April 1996. Lerner BH, Contagion and Confinement: Controlling Tuberculosis along the Skid Row (Baltimore 1998) Rosenkrantz BG, ed. From Consumption to Tuberculosis: A Documentary History (New York 1994); seed/soil quote by William Osler “Discussion on the Advisability of the Registration of Tuberculosis [1894] pg 317.
Submitted by Paul Colson, PhD, Program Director and Julie Franks, PhD, Health Educator and Evaluator Charles P. Felton National TB Center at Harlem Hospital
back to top
Staff Profile: John Bernardo, MD
TB Controller, Massachusetts Department of Public Health
Dr. John Bernardo is a very busy man: TB Medical Officer for Massachusetts, medical consultant for the RTMCC, Principal Investigator for the CDC TB Trials Consortium site at Boston University, co-Principal Investigator for the TB Epidemiology Consortium site at the Massachusetts State Laboratory, and Professor of Biochemistry and Medicine at Boston University. Not surprisingly, tracking John down for an interview was difficult.
When I finally caught up with him, I learned that John attended the University of Illinois and trained at NY Memorial Hospital and Boston City Hospital (BCH). After three years at the NIH as a Clinical Associate at the National Heart Lung And Blood Institute, John moved back to Boston and started working in the TB and allergy clinics at Boston City Hospital in 1979. “Carolyn Murray, the principal TB nurse at Boston City Hospital, is the one who really taught me about TB and public health,” John says, and he particularly admired her tenacity and patient-centered case management. Told by his boss in 1982 that he was replacing Ed Nardell as medical director of the BCH TB Clinic (Ed was moving on to bigger things), John’s been involved with TB ever since.
In the TB world, John is a past President of the National Tuberculosis Controllers Association (NTCA), and currently serves as the NTCA representative to the American Public Health Laboratory Steering Committee, as well as Chair-elect of Stop TB USA. John is perhaps equally famous for his work on the entertainment circuit at various TB and hospital functions. Past favorites include Connie Francis impersonations at Boston Medical Center, hula dancing in a grass skirt at the NTCA Conference, and going as the “Sultan of Swing” to a State TB Division party.
John sees TB patients at Quincy Medical Center and Pine Street Inn Shelter, as well as practicing pulmonary, critical care, and allergy medicine at Boston Medical Center. “He is a compassionate, caring clinician and someone who you can always count on to be there for the TB staff or for his TB patients – no matter what time of the day or night,” says Sue Etkind, Director of the Division of TB Prevention and Control at the Massachusetts Department of Public Health. Claire Murphy, the Nurse Practitioner who works with John at Pine Street, echoed a similar sentiment: “His easy way with the patients and his absolute respect for them makes our adherence rates go through the roof. No matter who you talk to, they will tell you how great he is.”
One of John’s favorite quotes is “Public Health is personal—one patient at a time,” and stories abound about how he lives up to this principle. Last Christmas Eve, a TB patient desperately wanted to be home with his family, but he needed Public Health clearance in order to go home. Despite having the day off, John heard that the public health nurse wasn’t going to be able to clear him before the holiday, so he drove out with Claire Murphy to clear the patient personally. “The patient was so happy to be with his family,” said Claire Murphy, “TB meds in hand, but celebrating Christmas at home.”
“I like TB because it’s personal. It gets to you because it affects people in more ways than other illnesses. And we still know so little about it,” says John. “The bacteria know more than we do,” but nevertheless John is committed to helping us humans try to catch up. John is invested in improving lab testing and understanding its ramifications in treatment, and serves as a frequent CDC consultant on matters regarding the use of inteferon gamma release assays (IGRA) tests to detect latent TB infection.
In what little spare time he has, John enjoys scuba diving in whatever ocean he happens to be by. “If he could conduct TB clinics under the sea, he would be in his glory!” says Claire Murphy.
Not dissuaded by a recent shark sighting off the Massachusetts coast, John was trying to catch a Bass ten feet underwater when he felt something latch onto his arm from above. Alarmed, he looked up and saw a huge black creature attacking his arm. As soon as the thrashing stopped and the creature let go, John quickly swam to the surface and looked around for the creature. He soon spotted his attacker, a black cormorant with ruffled feathers, floating on the surface and eyeing him deviously.
When he’s not diving or conducting NIH-funded research on intracellular signaling using flow cytometry, John can be found doing per diem car repair at a suburban Boston Toyota dealership. Sometimes patients bring their cars in for maintenance, only to find that their doctor is also their mechanic.
“I mostly do oil changes and replace windshield wipers,” John clarified. “They don’t let me do the big stuff.” He enjoys hanging out with the mechanics and learning from them, as well as chiding them about their smoking habit. Then he goes home and works on his beloved 1986 Volkswagon Scirocco with his collection of air tools. While John doesn’t have a car jack installed in his garage at home, the tone of his voice suggested that he hasn’t given up hope.
John’s automotive knowledge came in particularly handy about two years ago. “We had a very difficult patient who lived in an abandoned building and was a bit scary,” said Dr. Marie Turner, Medical Director of the TB Treatment Unit at Shattuck Hospital. “No one could get anywhere with him until John, upon meeting him, was able to strike up a conversation about an old car they had both owned in the past.” The patient was willing to have DOT after talking with John, but there was still one problem: No nurse felt comfortable going to the abandoned building to administer DOT. So John himself went out to give the man his medicines, always chatting about cars and bringing something for him to eat. “It was nothing short of a miracle,” Dr. Turner said. “John insisted the whole time that the patient was just a regular guy.”
John says the same thing about himself, but another scuba diving, hula dancing TB Medical Officer/auto mechanic has yet to emerge from the woodwork.
Submitted by Nickolette Patrick, MPH Health Educator, Northeastern RTMCC
back to top
Medical Consultation: GTBI Hosts National TB Expert Network Conference
In March 2008, the Centers for Disease Control and Prevention (CDC) proposed the concept of a national TB Expert Network Conference. The CDC identified the need for this conference during discussions with each of the four Regional Training and Medical Consultation Centers (RTMCCs) as part of their annual site visit. The MDR-TB Expert Network Meeting developed the Francis J. Curry Center to discuss MDR TB cases in California was an established model that could be promoted to a national level.
Therefore, the TB Expert Network Conference evolved as a joint project between the four RTMCCs, National Jewish Medical Research Center and CDC to provide a forum for expert consultants to discuss complicated treatment and case management issues and to foster training and capacity building among TB program medical consultants. Each of the collaborating Centers will be responsible for hosting one conference for a total of 6 conferences per year occurring on a bimonthly basis.
On May 13, 2008, the NJMS Global Tuberculosis Institute hosted the first web-based national TB Expert Network Conference. Two cases of MDR-TB and a review of relevant literature findings were presented by our physicians, Dr. Reynard McDonald and Dr. Alfred Lardizabal. The objectives of this conference were to discuss the basis for current recommendations for the management of MDR-TB and the challenges in application of these principles. Some of the key topics that were discussed included the use of an injectable agent in the treatment of MDR-TB, the role of surgical intervention, discrepancies in drug susceptibility testing results, the use of molecular methods for determining drug resistance, and the occurrence of cross resistance among the second line drugs.
There were 59 participants, including 31 physicians as well as several nurses and laboratory personnel. Based on the evaluations, strengths included the complexity of the cases, discussion among experts, participation from multiple sites, and diverse perspectives. Suggestions for improvement included presenting a single complicated case to allow more time for discussion and scheduling the conference on different days and times to accommodate the different schedules of individuals who wish to participate.
The second national TB Expert Conference was hosted by CDC on August 15, 2008. The Chuuk Epi Aid Team presented on the MDR-TB outbreak that occurred on the island of Chuuk in the Federated States of Micronesia. The conference discussed the nature of the outbreak and the challenges associated with treating and managing the MDR-TB cases and suspects (and associated contacts) in this setting. The next national TB Expert Network Conference will be hosted by the Southeastern National Tuberculosis Center on September 26, 2008 from 4:00-5:30pm EST.
Submitted by Anita Khilall, MPH Training and Consultation Specialist NJMS Global Tuberculosis Institute
back to top
Updated Monograph: Bringing the Science of Diagnosing LTBI to Practicing Clinicians
For more than 3 decades, treatment of persons with latent TB infection (LTBI) to prevent active TB disease has been an essential component of TB control in the United States. In 2002, a symposium was held in Miami Beach, Florida bringing together clinicians and researchers with considerable expertise on the diagnosis and treatment of LTBI. Each speaker prepared a paper touching upon on various aspects of the topic. As a result, a continuing medical education (CME) monograph summarizing the presentations was developed by GTBI to share with the greater clinician audience. This monograph, “Guidelines for the Diagnosis of Latent Tuberculosis Infection in the 21st Century,” was in great demand and eventually disseminated at a variety of clinical conferences.
In April 2008, GTBI released the 2nd edition of the monograph. This version includes updated versions of the chapters on the composition of tuberculin, a comparison of the 2 commercially available tuberculin solutions, a review of the literature on administration and interpretation of tuberculin skin tests, sensitivity to tuberculin by nontuberculosis mycobacteria, the role of the nurse in diagnosing LTBI, and a newly added paper on interferongamma release assays (IGRAs). This edition not only is certified for continuing medical education but for nursing contact hours as well.
We are also pleased to mention that the monograph is dedicated to Dr. George Comstock, one of the authors and, of course, a pioneer to whom we owe much of our knowledge in the field of TB. Dr. Comstock who passed away last year, saw to updating his chapter even while ill.
For view or to order the monograph, click here or call (973) 972-0979. Later this year, an online, interactive version will be available on the NJ Medical Global Tuberculosis Institute’s website.
Submitted by: Rajita Bhavaraju, MPH, CHES Training and Consultation Specialist NJMS Global Tuberculosis Institute
back to top
NE RTMCC Training Courses
Courses are open to participants in the 20 project areas (Maine, New Hampshire, Vermont, Massachusetts, Rhode Island, Connecticut, NJ, New York State, New York City, Pennsylvania, Michigan, Indiana, Ohio, West Virginia, Delaware, Maryland, Washington DC, Detroit, Baltimore, and Philadelphia) which are served by the Northeastern National Tuberculosis Center.
Individuals outside of this region who wish to attend our training courses, should first contact their Regional Training and Medical Consultation Center to check whether the same or similar course is being offered. If this is not the case, the out-of-region participant may then register for this course.
Click here for the list of upcoming courses.
back to top
TB Program Training Courses
Click here for the list of upcoming TB program courses.
back to top
What's New
 Promoting Cultural Sensitivity: A Practical Guide for Tuberculosis Programs That Provide Services to Persons from Somalia Published in August 2008 by CDC, this guide is designed to increase the knowledge and cultural sensitivity of health care providers, program planners, and any others serving persons from Somalia. This is the second in a series of 5 guides to help staff provide culturally competent TB care to some of our highest priority foreign-born populations. The first guide focused on persons from Laos. Other guides in the series will focus on persons from China, Mexico, and Vietnam. Each Guide includes (a) a two-page summary of program tips, (b) chapters on history and immigration; culture; health issues; and common perceptions, attitudes, and beliefs about TB, (c) a concluding summary, (d) appendices, including additional resources for working with TB patients and interpreters, and (e) references. All published guides can be accessed here.
Promoting Cultural Sensitivity: A Practical Guide for Tuberculosis Programs That Provide Services to Persons from Somalia Published in August 2008 by CDC, this guide is designed to increase the knowledge and cultural sensitivity of health care providers, program planners, and any others serving persons from Somalia. This is the second in a series of 5 guides to help staff provide culturally competent TB care to some of our highest priority foreign-born populations. The first guide focused on persons from Laos. Other guides in the series will focus on persons from China, Mexico, and Vietnam. Each Guide includes (a) a two-page summary of program tips, (b) chapters on history and immigration; culture; health issues; and common perceptions, attitudes, and beliefs about TB, (c) a concluding summary, (d) appendices, including additional resources for working with TB patients and interpreters, and (e) references. All published guides can be accessed here.
 Country Specific Guides for Healthcare Professionals Working with Foreign-Born TB Clients The Southeastern National Tuberculosis Center (SNTC) in collaboration with the Lung Health Center at the University of Alabama at Birmingham developed a series of TBspecific cultural competency guides. These individual country-specific guides (or summaries) include birth countries most commonly reported by foreign-born cases treated in the United States, namely Cambodia, Dominican Republic, Ecuador, Honduras, India, Mexico, Philippines, Somalia, and Vietnam. The series also includes an introductory guide. Each country guide (or summary) provides epidemiological information for both TB and HIV in each country, nicknames for TB, common misperceptions surrounding the etiology, disease transmission, and cures for TB and HIV as well as the stigma surrounding these diseases. A portion of the guide also provides information regarding polite greetings to use when meeting a person from this country, verbal and non-verbal communication, naming customs, cultural values, and internet links to translated educational materials for your clients. On August 27, 2008, the SNTC conducted a webinar on the Country Specific Guides that can be accessed here.
Country Specific Guides for Healthcare Professionals Working with Foreign-Born TB Clients The Southeastern National Tuberculosis Center (SNTC) in collaboration with the Lung Health Center at the University of Alabama at Birmingham developed a series of TBspecific cultural competency guides. These individual country-specific guides (or summaries) include birth countries most commonly reported by foreign-born cases treated in the United States, namely Cambodia, Dominican Republic, Ecuador, Honduras, India, Mexico, Philippines, Somalia, and Vietnam. The series also includes an introductory guide. Each country guide (or summary) provides epidemiological information for both TB and HIV in each country, nicknames for TB, common misperceptions surrounding the etiology, disease transmission, and cures for TB and HIV as well as the stigma surrounding these diseases. A portion of the guide also provides information regarding polite greetings to use when meeting a person from this country, verbal and non-verbal communication, naming customs, cultural values, and internet links to translated educational materials for your clients. On August 27, 2008, the SNTC conducted a webinar on the Country Specific Guides that can be accessed here.
 Community Involvement in TB Care and Prevention: Towards Partnerships for Health This WHO publication provides guiding principles for countries to promote the involvement of people with TB and the community in TB care and prevention. These recommendations are designed to support health policy-makers – and patients’ groups and local partners – in including community involvement activities in national strategic plans to control TB. The recommendations also offer advice on how to fund this work and successfully scale up approaches that have worked effectively.
Community Involvement in TB Care and Prevention: Towards Partnerships for Health This WHO publication provides guiding principles for countries to promote the involvement of people with TB and the community in TB care and prevention. These recommendations are designed to support health policy-makers – and patients’ groups and local partners – in including community involvement activities in national strategic plans to control TB. The recommendations also offer advice on how to fund this work and successfully scale up approaches that have worked effectively.
.
back to top
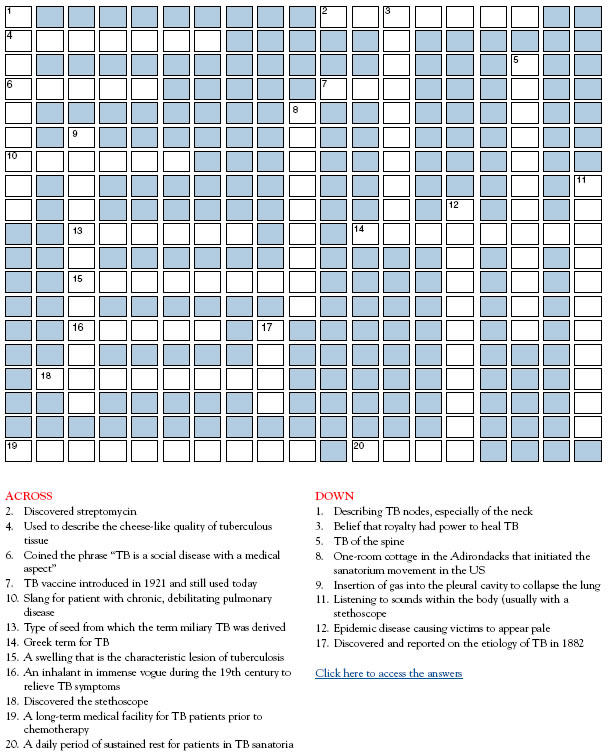
TB Puzzler
(Try your hand at TB terms and medical leaders from an earlier era)
[Please print this page]
back to top
Links - Other TB Resources
Division of Tuberculosis Elimination
The mission of the Division of Tuberculosis Elimination (DTBE) is to promote health and quality of life by preventing, controlling, and eventually eliminating tuberculosis from the United States, and by collaborating with other countries and international partners in controlling tuberculosis worldwide.
TB Education and Training Resources Website
This website is a service of the Centers for Disease Control and Prevention (CDC), Division of Tuberculosis Elimination. It is intended for use by TB and other healthcare professionals, patients, and the general public and can be used to locate or share TB education and training materials and to find out about other TB resources.
TB Education & Training Network (TB ETN)
The TB Education and Training Network (TB ETN) was formed to bring TB professionals together to network, share resources, and build education and training skills.
TB-Related News and Journal Items Weekly Update
Provided by the CDC as a public service, subscribers receive:
- A weekly update of TB-related news items
- Citations and abstracts to new scientific TB journal articles
- TB conference announcements
- TB job announcements
- To subscribe to this service, click here
TB Behavioral and Social Science Listserv
Sponsored by the DTBE of the CDC and the CDC National Prevention Information Network (NPIN), this Listserv provides subscribers the opportunity to exchange information and engage in ongoing discussions about behavioral and social science issues as they relate to tuberculosis prevention and control.
New England Tuberculosis Prevention and Control Website
At the beginning of 2005, the six New England TB Programs joined together to promote a regional approach to TB elimination. This web site represents a step toward building collaboration, exchanging experiences and practices, and enhancing program capacity.
Other RTMCCs
The Curry International Tuberculosis Center serves: Alaska, California, Colorado, Hawaii, Idaho, Montana, Nevada, Oregon, Utah, Washington, Wyoming, Federated State of Micronesia, Northern Mariana Islands, Republic of Marshall Islands, American Samoa, Guam, and the Republic of Palau.
The Heartland National Tuberculosis Center serves: Arizona, Illinois, Iowa, Kansas, Minnesota, Missouri, New Mexico, Nebraska, North Dakota, Oklahoma, South Dakota, Texas, and Wisconsin.
The Southeastern National Tuberculosis Center serves: Alabama, Arkansas, Florida, Georgia, Kentucky, Louisiana, Mississippi, North Carolina, South Carolina, Tennessee, Virginia, Puerto Rico, and the U.S. Virgin Islands.
back to top
Key Contacts
- Lee B. Reichman, MD, MPH - Executive Director
- Reynard J. McDonald, MD - Medical Director
- Bonita T. Mangura, MD - Director of Research
- Eileen C. Napolitano - Deputy Director
- Nisha Ahamed, MPH, CHES - Program Director, Education and Training
- Chris Hayden - Northeastern Spotlight Editor
- Alfred S. Paspe - User Support Specialist/Webmaster